Peripheral Arterial Disease (PAD) is a condition which affects approximately 12 million people in the United States. The disease results from the accumulation of plaque in arteries, most commonly occurring in the pelvis and legs. PAD occurs when plaque buildup causes a narrowing of the artery, constricting normal blood flow to the body’s tissue and organs. If left untreated, PAD increases the risk of heart attack, stroke, amputation and death. In fact, whether they are symptomatic or not, patients with PAD face a five-year mortality rate of 30%. An estimated 12 million people in the U.S. have peripheral arterial disease (PAD). However, PAD is often undiagnosed or misdiagnosed because patients are either asymptomatic or dismiss their symptoms as part of the normal aging process.
Symptoms of PAD include, but are not limited to, the following:
If a patient has symptoms associated with PAD, several tests can be performed to make a diagnosis. An ankle brachial index (ABI) is used to measure the rate of blood pressure in the ankle to that in the arm. A lower pressure in the ankle may indicate PAD. This is a simple, non-invasive test, which can be done in the doctor’s office. Another non-invasive test called a Doppler Ultrasound, uses sound waves to measure blood flow in a vessel and can determine if there is a blockage.
To make a final assessment, angiography is performed. This minimally invasive procedure involves injecting a dye into the arteries and reviewing the area by X-Ray. Typically, the physician can see the blockage on the angiogram images.
Researchers have identified certain risk factors, which can contribute to the development of peripheral arterial disease. Key risk factors include:
Additional risk factors include hypertension, high cholesterol, obesity and family history.
If left untreated, PAD can progress to critical limb ischemia (CLI), which occurs when there is not enough oxygenated blood being delivered to the leg to keep the tissue alive. An estimated 750,000 people in theUnited States suffer from CLI, which occurs when symptoms of PAD including pain, non-healing wounds, tissue loss or gangrene become more severe.1
When CLI develops, it can lead to constant pain and even amputation of toes, feet and/or part of the leg. Within one year of the onset of CLI, 25% of patients will die and another 25% will require major amputation. Last year, over 150,000 amputations were performed in the U.S. and Europe, with a 40% mortality rate at two years post-amputation.
A number of options are available for treating PVD, including surgery and non-surgical treatments, such as angioplasty and vascular stent placement.
In the past, surgery was the only treatment available for PVD and, in some cases, surgery may still be needed. When surgery is required, the surgeon implants a new vessel (a natural or synthetic vascular graft) that allows blood to bypass the obstruction. The procedure usually requires one or more incision to perform.
In recent years, a new non-surgical procedure called percutaneous transluminal angioplasty (PTA) has been performed on patients with PVD. During angioplasty, a specially trained doctor inflates a tiny balloon inside the vessel, compressing the plaque against the vessel walls. The balloon then deflates and is withdrawn from the vessel. This procedure is performed entirely within the vessel through a small puncture in the skin. However, because angioplasty does not always restore blood flow effectively, the doctor may recommend placement of an intravascular stent in the vessel.
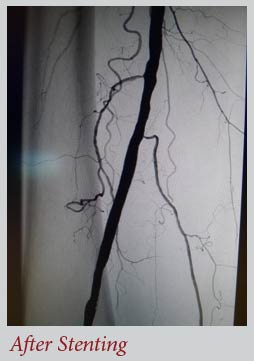
An intravascular stent is a small stainless steel tube that is introduced into the blocked artery. The stent is then gently expanded to open the vessel, restore blood flow, and relieve symptoms. The stent remains in the vessel as a permanent implant. The stent is placed on the balloon catheter and directed to the blocked area of the vessel. Once the balloon and stent are in the correct position, the balloon is inflated, causing the stent to open. One or more stents may be expanded in the vessel. The stent will remain in place permanently, keeping the vessel open. The healthy lining of the vessel will slowly grow over the stent, permanently incorporating it into the vessel wall. The stent will not limit daily activities in any way, and sent patients can almost always return to their normal activities. Patients who have had a vascular stent implant should tell this to any doctor who treats them in the future.

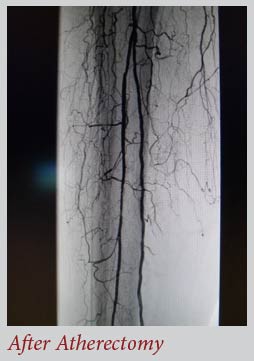
Why some arteries treated with stents and angioplasty re-close quickly while others stay open indefinitely remains to be completely understood. The SilverHawk® Plaque Excision System is a device used to remove plaque that commonly blocks arteries and interrupts blood flow. Unlike stenting and other methods of opening the artery, the SilverHawk removes the source of the problem plaque build-up instead of simply compressing it against the vessel wall. Atherectomy can also be achieved by using a cool laser (Spectranetics) that vaporizes the blockages restoring blood flow.
When the blockage is difficult to reach or the plaque becomes “calcified,” theDiamondback 360® uses a tiny, rotating diamond-coated “crown” inserted into the artery that gently sands away tough plaque and restores blood flow.